

INTRODUCTION
Coronavirus illness 2019 (COVID-19) has had a huge impact worldwide as a results of the mode of infection spread, the ensuing severe acute respiratory syndrome, and therefore the international death toll.
The commonest clinical symptoms are fever, headache, sore throat, dyspnea, dry cough, abdominal pain, vomiting, and diarrhea.
The implications of spit for virus transmission and the chance of salivary glands as a reservoir, few oral manifestations are reported.
- Oral dryness
- Vesiculobullous lesions
- Aphthous‐like lesions
- Dysgeusia and
- Anosmia are the foremost common oral signs reported
ACE2 MEMBRANE IN ORAL CAVITY
ACE2 has been found in oral mucous membranes, particularly with more density on dorsum of tongue and secretion glands relative to buccal mucosa or palate.
The S macromolecule binds to ACE2 and is activated by the serine transmembrane peptidase 2.
High expression of this enzyme has been known in numerous areas of the human body, corresponding to in respiratory organ alveolar epithelial cells sort II (AT2), heart muscle cells, mouth mucosa, upper esophagus stratified epithelium, ileum, and colon enterocytes, cholangiocytes, proximal kidney tubule cells, and urothelial cells of the bladder.
TASTE ALTERATION (DYSGEUSIA) AS A MAJOR SIGN
Taste alteration has been reported as an early sign of SARS-CoV-2 infection in adults.
Expression of ACE2 is the main issue for viral entry into the host cell in SARS-CoV-2 infection.
ACE2 is expressed in epithelial cells from completely different sites within the mouth. The very best expression was found in the tongue and lesser amounts in the oral and gingival tissue.
Expression of ACE2 has additionally been detected in secretion glands, that may determine the oral cavity as an extremely vulnerable site for SARS-CoV-2 infection. although the mechanism for the alteration in the perception of taste by this coronavirus isn't clear, this symptom might be thought of an early manifestation in infected adults.
The viral lytic pathway may conjointly directly have an effect on the peripheral neuronal flight of the sensation tract in two ways:
- Direct harm of ACE2-expressing cells of the style buds and peripheral taste neurosensory chemoreceptors, or
- Direct damage of any of the cranial nerves to blame for gustation (CN VII, IX, or X). Among these, damage to chorda tympani (CN VII) may well be the foremost plausible explanation: Once the nasopharynx is colonized, SARS-CoV-2 virus could use the auditory tube as a port of entry and colonize the center ear, inflicting resultant damage to the chorda tympani and therefore the resultant dysgeusia.
SARS-CoV-2 virus binds to ACE2 receptors present within the oral mucosa, triggering an associated inflammatory response that results in cellular and genetic changes that might alter taste.
Inflammatory cytokines, appreciate IFN (interferon) will trigger programmed cell death and thus may cause abnormal turnover in taste buds, which can lead to net losses of taste bud cells and/or skewing the illustration of various kinds of taste cells and ultimately cause the event of taste dysfunction.
The time of onset of dysgeusia may correspond with the time when zinc supplementation in the form of lozenges or syrups may be most effective because this localized delivery of zinc to oral and oropharyngeal mucosa may help control COVID-19 replication at early replication sites.
APHTHOUS LIKE ULCERS
Aphthous‐like lesions appeared as multiple shallow ulcers with erythroderma halos and yellow‐white pseudomembranes on the each keratinized and nonkeratinized tissue layers.
Increased level of tumor necrosis factor (TNF)‐α in COVID‐19 patients will result in chemotaxis of neutrophils to oral mucosa and development of aphthous‐like lesions.
Stress and immunosuppression secondary to COVID‐19 infection might be alternative attainable reasons for the look of such lesions in COVID‐19 patients.
The ascertained lesions exhausted most of the covid patient is given two well-defined and distinct patterns, one resembling aphthous-like ulcers in young patients with delicate cases of COVID-19 and another with a lot of widespread patterns resembling herpes simplex 1 necrotic ulcers within the a lot of severe and immunological disorder older individuals.
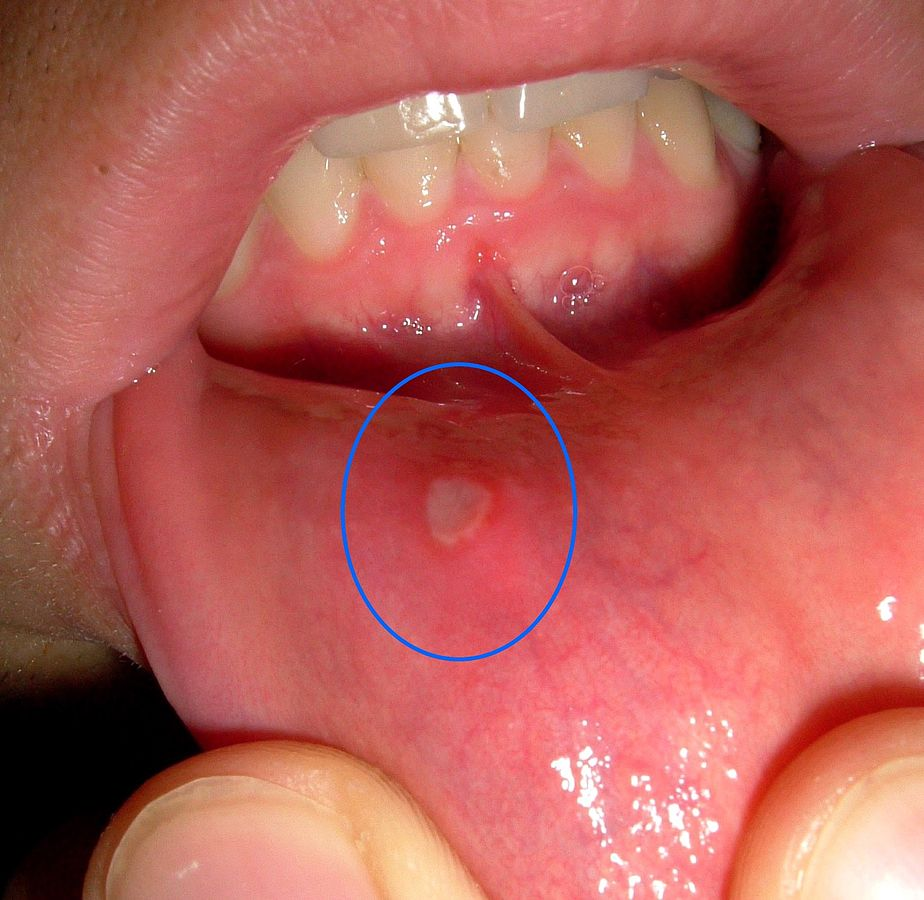
Photo credit: Maksim (wikipedia commons)
ULCERATIVE AND EROSIVE LESION
Ulcerative or erosive lesions appeared as painful lesions with irregular borders on the tongue, hard palate, and labial mucosa.
It would be reported by the thousands of symptomatic patients who have been laid low with the unwellness as a result of oral ulcers that are terribly painful and interfere with chewing, swallowing, and speaking.
In research articles reported, a patient with tongue inflammation throughout the primary 24 h, with future evolution to an erythematous macula, that resulted in an irregular and symptomless ulcer.
The lesion in all probability derived from an inflammatory reaction triggered by inflammation caused by COVID-19Different factors together with drug eruption (to anti-inflammatory in one case), vasculitis, or thrombotic vasculopathy secondary to COVID‐19 were advised as causes for development of lesion and erosive lesions.
Additional studies have to be compelled to investigate whether or not SARS-CoV-2 infection directly causes oral ulcerations or whether oral lesions are a synchronic event with COVID-19 progression.
ORAL HERPETIC LESIONS AND PETECHIAE
Herpes zoster (HZ) is caused by the varicella‐zoster virus, that reactivates and spreads from the dorsal root ganglia to its several dermatomes.
Patients in danger of Hertz embrace elders and upset hosts. truly clinical manifestation of COVID‐19 itself, being a herpes zoster‐like lesion.
Though we tend to don't contemplate that the symptoms of varicella and herpes zoster are caused solely by COVID‐19, the event of symptoms will be promoted by the expression of Varicella zoster virus in COVID‐19.
Geographic tongue appeared when recovery of herpetiform lesions. Stress and immunological disorder related to COVID‐19 was the prompt cause for the look of secondary herpetic gingivostomatitis.
Petechiae were reported on the lower lip, palate, and oropharynx mucosa.
Latency time for patients with petechiae was shorter compared to the patients with each petechiae and macular lesions. blood disorder because of COVID‐19 infection or the prescribed drug were prompt as potential causes of petechiae.

ORAL DRYNESS
Dry mouth could be a disorder that happens because of inadequate saliva secretion or absolute salivary gland dysfunction.
Patients with COVID-19 who described dryness as a primary criticism that generally continued over the course of the disease. During this study, xerostomia (dry mouth) was reported in patients with COVID-19.
The ACE 2 and TMPRSS 2 receptors have a stimulating expression within the epithelial cells of salivary glands. Therefore, it appears that these glands are appropriate receptors for SARS-CoV-2 and are among the primary target cells of this virus and doubtless the virus will simply enter the salivary glands leading to infection.
Inflammatory and infectious procedures are noted as factors influencing reduced saliva. Anxiety and worries concerning being affected by disease and hospitalization can be thought of as background factors for dry mouth in patients.

ANOSMIA
Hyposmia and anosmia are symptoms usually detected by COVID-19 patients. Olfactory neurons are mentioned as a portal of entry for neuroinvasion by CoVs, which can be transferred to the central nervous system via a synapse-connected route.
Still it's unclear whether or not modality sensory neurons are directly concerned within the pathological process of smelling loss in COVID-19.
Some patients have conferred entirely with this symptom, and first physicians and otolaryngologists have to be compelled to bear in mind this putative presentation.

CONCLUSION
Though oral manifestation is one of the important symptoms dentists also put forward to monitor these symptoms and helpful to overcome this pandemic coronavirus as because the first portal of entry is the mouth that is oral cavity.
REFERENCE
- Díaz Rodríguez M, Jimenez Romera A, Villarroel M. Oral manifestations associated with COVID-19 [published online ahead of print, 2020 Jul 22]. Oral Dis. 2020;10.1111/odi.13555. doi:10.1111/odi.13555
- Iranmanesh B, Khalili M, Amiri R, Zartab H, Aflatoonian M. Oral manifestations of COVID-19 disease: A review article. Dermatol Ther. 2021;34(1):e14578. doi:10.1111/dth.14578
- Al-Khatib A. Oral manifestations in COVID-19 patients. Oral Dis. 2021;27 Suppl 3:779-780. doi:10.1111/odi.13477
- SARS-CoV-2 impact on oral health: a general view. Bol Med Hosp Infant Mex. 2021;78(2):91-94. doi: 10.24875/BMHIM.20000192.
- Brandão TB, Gueiros LA, Melo TS, et al. Oral lesions in patients with SARS-CoV-2 infection: could the oral cavity be a target organ?. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021;131(2):e45-e51. doi:10.1016/j.oooo.2020.07.014.
- de Carvalho LFDCES, Kitakawa D, Cabral LAG. Oral lesions of herpes zoster in COVID-19 patients or truly associated to the disease?. Oral Dis. 2021;27 Suppl 3:774-775. doi:10.1111/odi.13472
- Fathi Y, Hoseini EG, Atoof F, Mottaghi R. Xerostomia (dry mouth) in patients with COVID-19: a case series. Future Virol. 2021;10.2217/fvl-2020-0334. doi:10.2217/fvl-2020-0334.
- Hornuss D, Lange B, Schröter N, Rieg S, Kern WV, Wagner D. Anosmia in COVID-19 patients. Clin Microbiol Infect. 2020;26(10):1426-1427. doi:10.1016/j.cmi.2020.05.017









0 Comments