

INTRODUCTION
self‐contained underwater breathing apparatus (SCUBA) diving, general dental practitioners ought to be ready to deal with complications arising as a results of diving and to produce patients with correct data.scuba diving could trigger issues in some parts of the body such because the nose, ear, lung, and temporomandibular joint.
Although diver's mouth syndrome (DMS) has long been recognized by breathing device divers, very little attention has been paid to the influence of sporting a scuba diving mouthpiece on the stomatognathic system.
The ideas of diving drugs and dental medicine to the dentist, and to produce the dentist with some diagnostic tools yet as treatment guidelines.
Dental symptoms in recreational breathing device divers and describe the distribution of those symptoms on the premise of diver demographics, diving qualifications and dive conditions throughout the episode of dental pain
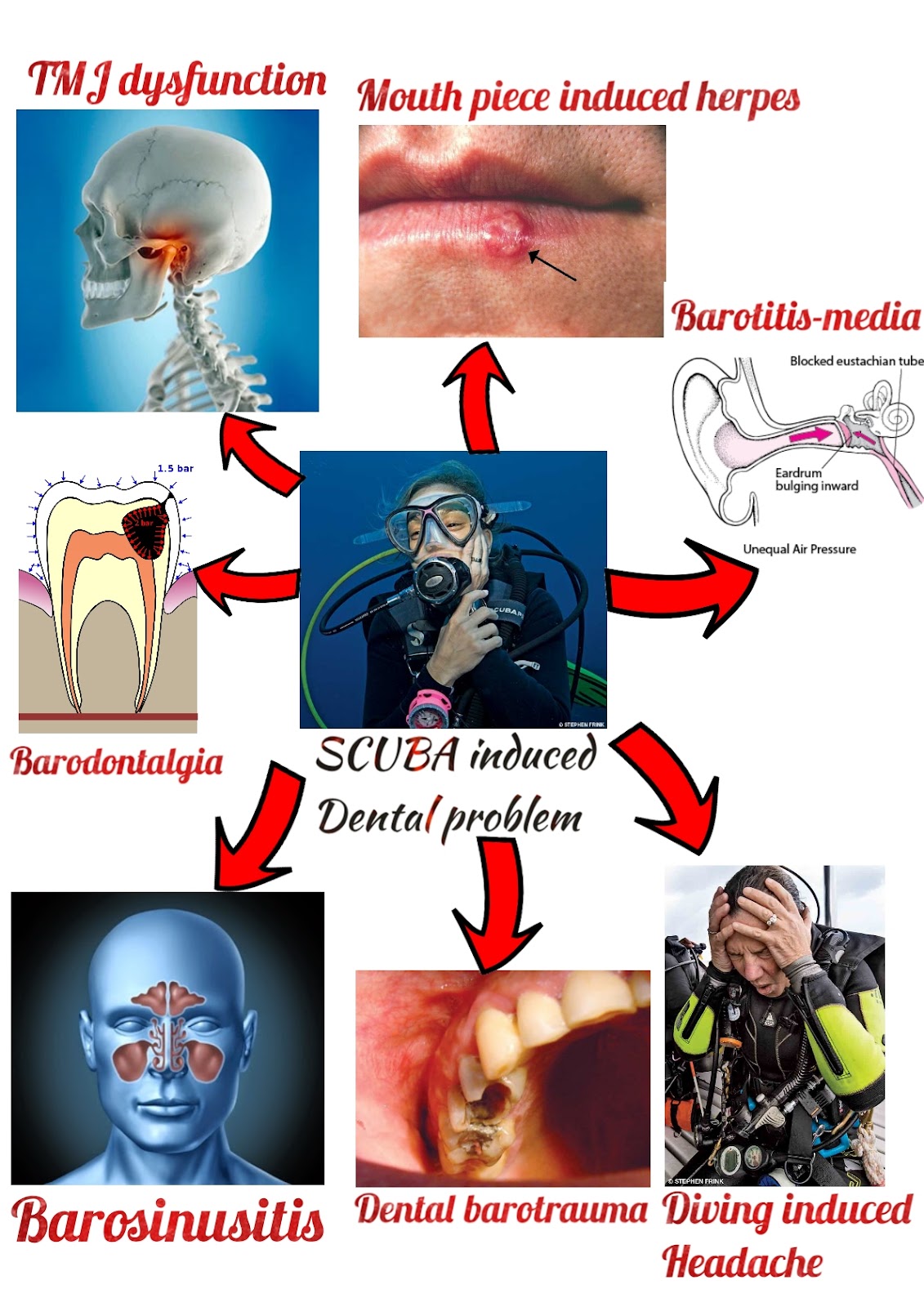
SCUBA INDUCED DENTAL PROBLEM
Barotrauma (pressure‐induced injury concerning an air space) to the head, face and oral regions, additionally as breathing device mouthpiece‐related oral conditions.The relevant conditions for dentists are
- Diving‐associated headache (migraine, tension‐type headache)
- Barosinusitis and barotitis‐media (sinus and tympanic cavity barotrauma, respectively)
- Neuropathy, cranial nerve (CN V) or facial (CN VII)
- Nerve baroparesis (pressure‐induced palsy)
- Dental barotrauma (barometric‐related tooth injury)
- Barodontalgia (barometric‐related dental pain)
- Mouthpiece‐associated herpes infection
- Pharyngeal gag reflex
- Articulatio temporomandibularis disorder (dysfunction).
DENTAL COMPLICATIONS OF MOUTHPIECE
The diving mouthpiece has obvious connection to oral tissues and conditions. The scuba diver gets air from a compressed gas tank, that is transmitted to the mouth via a regulator with a mouthpiece that's control by the teeth (usually the canines and premolars). associate airtight seal must be created between teeth and lips. Inability to carry the mouthpiece because of complete or partial edentulism is one amongst the contraindications for skin-dive.There are 3 mouthpiece designs:
- Industrial
- semi‐customized
- customised mouthpieces.
The air pushing by mouthpiece into post‐surgical wound might induce intraoral pain, mimicking barodontalgia. due to the Helium in Aqua-Lung tanks and therefore the ensuing lower gas viscousness, air from the pressurised tanks will be forced in through carious lesions and defective margins of restorations also.
The diving mouthpiece as a attainable vector for transmission of herpes simplex virus between mates, particularly throughout underwater drills, during which the mouthpiece is changed often between participants to simulate emergency conditions.

SCUBA diving mouth piece
Photo credit: https://www.okdiversbali.com/blog/mouthpiece-diving-regulator
DIVING RELATED HEADACHE
Barotrauma‐related headache of 15–20minute length was according throughout ascending and descending.Distribution between unilateral and bilateral headache was nearly equal, and regarding one‐fifth of those headaches were diagnosed as migraine.
Indeed, weather and barometrical changes are usually thought-about as major headache triggers by migraine patients.
Headache may additionally be a manifestation of decompression sickness (DCS), within which speedy ascent with rapid decompression permits the discharge of dissolved nitrogen and therefore the creation of gas bubbles with probably severe consequences in varied body organs (e.g. joint pain, skin rash, itching, dizziness, nausea, vomiting, symptom and fatigue).
BARO SINUSITIS
Barosinusitis is an acute or chronic inflammation of 1 or a lot of of the cavity sinuses, created by the event of a pressure difference between the air within the sinus cavity which of the encircling atmosphere.The pressure gradient created ends up in a vacuum, which can cause tissue layer swelling, serosanguinous exudate and submucosal hematoma.
These ailments might consequently cause pain, generally abrupt and severe, and presumably bleeding.
Palsy might occur as a results of ischemic neurapraxia of branches of the fifth cranial nerve within the maxillary sinus.
The incidence of barosinusitis during diving descent is regarding double that in ascent.
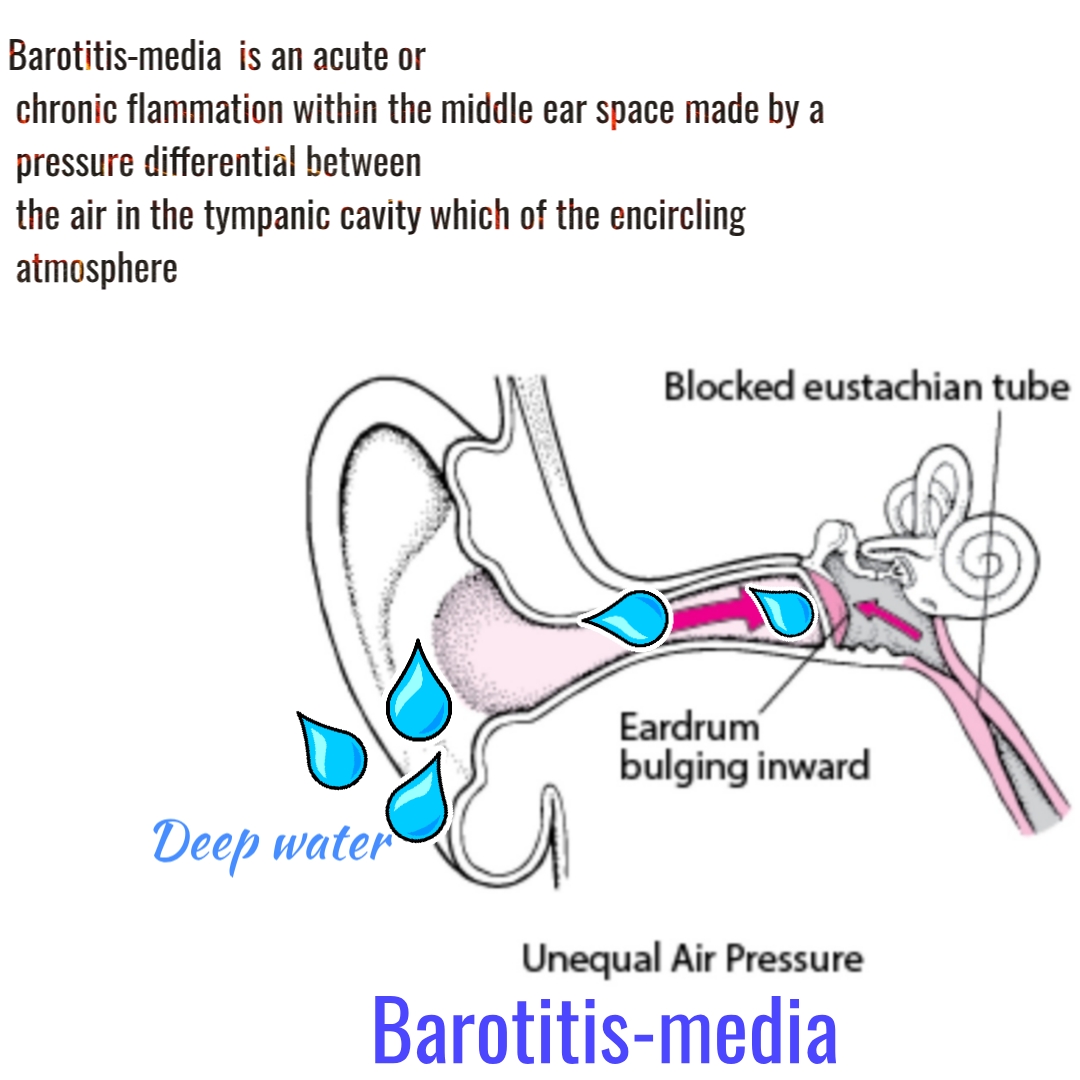
BAROTITIS MEDIA
Barotitis‐media is an acute or chronic flammation within the middle ear space made by a pressure differential between the air in the tympanic cavity which of the encircling atmosphere.The symptoms of barotitis‐media vary from ear discomfort to intense earache, tinnitus, vertigo with nausea, and deafness.
A possible complication is facial palsy secondary to tympanic cavity barotrauma, caused once elevated pressure from the center ear is transmitted to the facial canal via dehiscence inside its course on the medial wall of the middle ear or via the orifice of the chorda tympani, leading to ischemic neurapraxia of the cranial nerve.
This development sometimes happens solely on one episode, even in people who are recurrently exposed to similar barometric conditions.
The condition is unilateral, occurring throughout or shortly once diving ascent, with the potential involvement of facial features muscles and gustatory sensation from the anterior tongue.
Spontaneous resolution sometimes happens inside a brief time, as blood flow quickly resumes when pressure within the tympanic cavity becomes below capillary closing pressure.
DENTAL BAROTRAUMA
According to Boyle’s Law, the volume of gas at constant temperature varies inversely with the surrounding pressure. The changes in gas volume within the body’s rigid cavities, related to the ever-changing atmospheric pressure, will cause many adverse effects, that are noted as barotraumaDental barotrauma will manifest as tooth fracture, restoration fracture and reduced retention of dental restoration.
The term barodontocrexis describes the phenomenon of dental fracture.
Dental barotrauma happens whereas ascending; upon egress once finishing the dive, the diver might report that a tooth bust or has shattered.
Dental barotrauma will seem with or while not pain kind of like dental fracture occurring at ground level.
Other than want for dental treatment, potential consequences embrace aspiration or swallowing of the dislodged restoration or dental fragment, and pain, which can cause incapacitation whereas diving and premature ending of the planned dive.
The predisposing factors that appeared repeatedly in dental barotrauma reports were pre‐existing leaked restoration and/or occult remaining/recurrent cavity lesions beneath restoration within the affected tooth before exposure to the measuring system changes.
Pressure changes in small air bubbles within the cement layer beneath crowns will cause a major reduction of the prosthetic device’s retention and even to removal, particularly if the crown was cemented with Zn phosphate cement.
- The crowns that were cemented with either Zn phosphate cement or glass‐ionomer cement had considerably reduced retention
- The mechanism of removal is because of porosities generated throughout the preparation of Zn phosphate cement and glass‐ionomer cement, and also the enlargement and contraction of those microbubbles upon pressure changes cause weakening of the cement. Indeed, microleakage was detected within the Zn phosphate and glass‐ionomer cements once pressure sport, whereas no microleakage was detected within the resin cement, in all probability due to dentinal tube obstruction by resin tags or cement flexibility.
- The dental practitioner ought to perform preventive measures and sporadically examine his or her patients who dive and look for occult pathologies, equivalent to leaked restorations and secondary cavity lesions.
- Since dislodged partial removable prostheses can be accidentally aspirated throughout diving (with one rumored case of ensuing death), these devices ought to be removed before diving, unless they're firmly preserved.
- Retention by adequate osteointegrated dental implants is perhaps the most effective resolution for edentulous diverse.
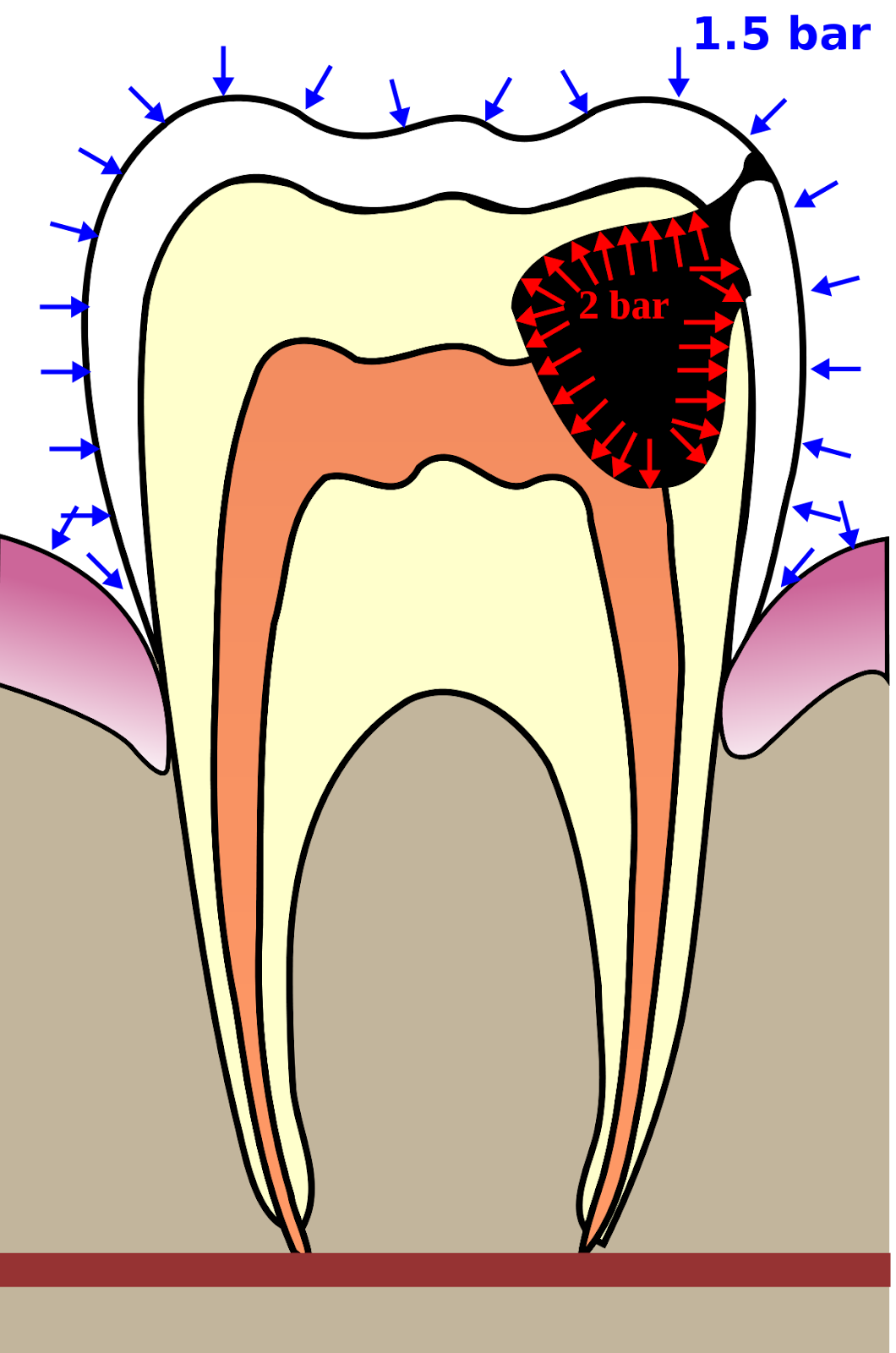
Pressure induced in tooth black colour indicators caries

Due to increase in pressure amalgam restoration dislodged
BARODONTALGIA
Barodontalgia also called odontalgia is outlined as a barometric pressure-induced oral pain, which can be dental or non dental.Barodontalgia is one in all these undesirable effects and is expounded to atmospheric pressure changes.
This is condition is generally a signal of pre-existing oral or maxillofacial malady.
The exact mechanism of pain continues to be unclear.
This pain development are often divided to 2 categories, particularly direct barodontalgia and indirect barodontalgia.
- The indirect sort is of non-dental origin (e.g., barosinusitis, barotitis-media)
- The direct pain is of dental origin, admire recent dental medical care, deep decay and leaky restorations, and pulpitis.
The look of pain on ascent is sometimes relating to pulpitis and appearance on descent to necrotic pulp diseases or facial barotrauma.
Pain from peri-radicular pathology might seem throughout descent or ascent.
Most of the cases of pain happen throughout ascent.
Pain sometimes ceases once returning to onset level or ground atmospheric level, however might linger if originating from Peri-radicular pathology or facial barotrauma
Dental care includes,
- The present low rate are often attributed to cabin pressurization, fluoridisation of drink and oral hygiene product, that result in reduced dental morbidity, and higher dental care.
TMD DYSFUNCTION
TMD symptoms were a lot of prevailing in diving in cold water than in warm water, in all probability attributable to the impairment of the lips’ acquiring capability within the cold surroundings, therefore implementing over‐effort of the masticatory muscles.Diving connected TMD symptoms ought to be differentiated from barotitis symptoms.
TMD was the second most prevailing head and neck disorder per Zealand diverse
TMD was the second most prevailing head and neck disorder per Zealand diverse
Diver’s mouth syndrome may embrace all the TMD symptoms appreciate muscle pain, joint pain, internal derangement of TMJ‐disc, headache in numerous degrees, and will be restricted to diving time or become chronic and constant.
These symptoms are attributed to the protruded mandibular position and therefore the biting force exercised on the anterior occlusion (usually canines and premolars) throughout diving.
A semi‐customized mouthpiece needed less muscle activity for retention than business kind, and totally custom-made mouthpieces are rumored to cause the smallest amount mandibular displacement from the normal resting position, therefore usage leads to the smallest amount discomfort, muscle pain, fatigue and energy.
To prevent post‐surgical forcing of air into the tissues and inflammation, diving ought to be restricted for a minimum of one week following oral surgery before diving the dentist should ensure healing.
Hobson and Newton counseled the fabrication of a custom mouthpiece for diverse, with a bite platform a minimum of 4mm in thickness, particularly for diverse who expertise diving‐associated TMD symptoms.
The dentist should educate the diver patient the infectious potential of the mouthpiece and advocate using solely a non-public one, and encourage maintenance by hygiene procedures once every use, like alternative removable oral devices.

REFERENCE
Special thanks to Yehuda Zadik, Hadassah Medical Center. Most of the references taken from his article only
- Zadik, Yehuda & Drucker, S. (2011). Diving dentistry: A review of the dental implications of scuba diving. Australian dental journal. 56. 265-71. DOI:10.1111/j.1834-7819.2011.01340.x
- https://www.diversalertnetwork.org/health/ears/tmj-temporamandibular-joint-syndrome.
- Nakdimon, Idan & Zadik, Yehuda. (2019). Barodontalgia Among Aircrew and Divers: Meta-analysis. Aerospace Medicine and Human Performance. 90. 128-131. 10.3357/AMHP.5183.2019.
- Grossman A, Ulanovski D, Barenboim E, Azaria B, Goldstein L. Facial nerve palsy aboard a commercial aircraft. Aviat Space Environ Med 2004;75:1075–1106.
- Stewart TW Jr. Common otolaryngologic problems of flying. Am Fam Physician 1979;19:113–119.
- Hyams AF, Toynton SC, Jaramillo M, Stone LR, Bryson PJ. Facial baroparesis secondary to middle‐ear over‐pressure: a rare complication of scuba diving. J Laryngol Otol 2004;118:721–723
- Zadik Y. Dental barotrauma. Int J Prosthodont 2009;22:354–357
- Hanna HH, Thomas‐Yarington C. Otolaryngology in aerospace medicine. In: DeHart RL, ed. Fundamentals of Aerospace Medicine. Philadelphia: Lea and Febiger, 1985:525–536.
Photo taken from
- https://www.medicinenet.com/temporomandibular_joint_syndrome_tmj/article.htm#
- http://www.alertdiver.com/Unexpected-Air-Pockets
- https://doi.org/10.14219/jada.archive.2009.0338
- http://impocity.blogspot.com/2015/03/aerosinusitis-or-barosinusitis.html
- https://en.m.wikipedia.org/wiki/Herpes_labialis
- http://www.alertdiver.com/Diving_After_DCS









1 Comments
Just wanted to say I love reading your blog. we provide 24 Hour Emergency Dentist Philadelphia at affordable prices. for more info visit our website.
ReplyDelete